

Duty of Care or Overreach? Legal Risks in Gender Transitioning Students
Duty of Care or Overreach? Legal Risks in Gender Transitioning Students
Examining the Legal Implications of Duty of Care in Gender Transitioning Children

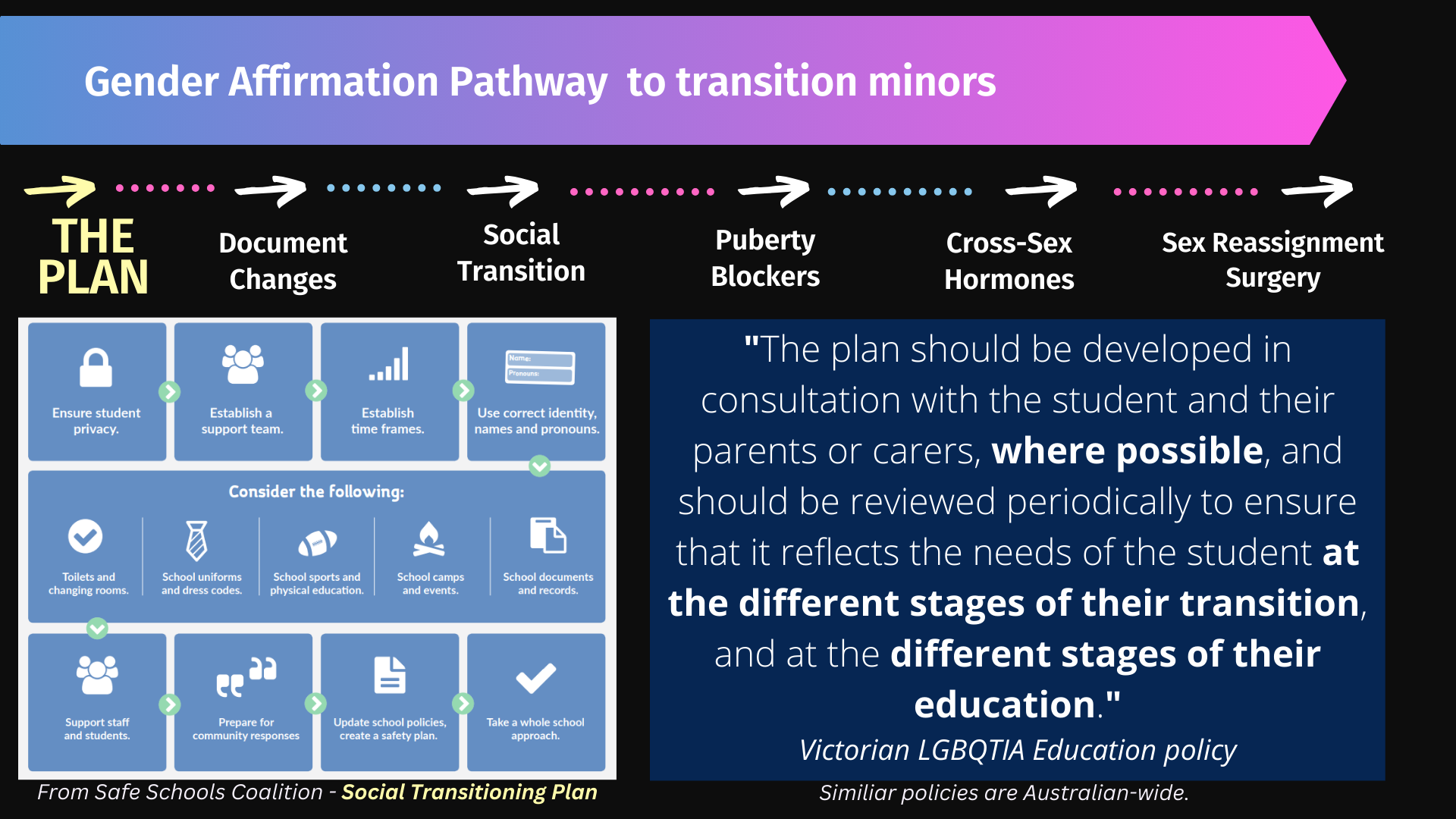
Gender Identity Ideology (GII) posits the idea that some people have been born in the wrong body and should have been born the opposite sex. This can lead to a person presenting as the opposite sex (otherwise known as Social Transition) and undertaking medicalisation and surgeries to further enhance their transition (known as Gender Affirming Care). Most schools in Australia have included GII in their curriculum. Many schools are supporting Social Transition, and some are actively hiding the Social Transition of a child from the child’s parents.
Schools supporting GII usually have policies that include overtly displaying trans/pride flags, forcing students to use pronouns different to the biological sex of another student, forcing students to use gender neutral toilets, allowing boys to play on girls sports teams and be involved in girls activities (and vice versa).
Evidence is mounting that Social Transition is not a neutral act but an active intervention. (see this article on the Cass Review UK)1. Children who are allowed to Socially Transition almost always proceed to Gender Affirming Care. Those children who are not allowed to Socially Transition mostly grow out of any issues they had with their gender. See analysis of current studies here2.
The children who proceed to Gender Affirming Care are treated by the medical profession with medicines and surgeries to try and make them look like the opposite sex. These are given to the child without any investigation into the reasons for the desire to appear as the opposite sex. The child is making the diagnosis and the medical profession merely “affirm” that diagnosis.
The drugs and hormones given are:
1. Puberty Blockers for children beginning puberty. These are spruiked as “halting” puberty to allow the child to decide which sex he/she would like to be. However, the evidence shows that the drugs stop puberty, and the child misses crucial developmental stages leading to sterilisation, lack of proper cognitive development, osteoporosis, lack of sexual function and many other catastrophic irreversible side effects. See HERE3 for more details.
2. Testosterone. Females are given high doses of testosterone to bring on male characteristics. The voice lowers, hair sprouts in a male pattern way and muscle and fat are reorganised. These are the wanted effects, but the other effects caused by giving a female body hormones for which it is not designed are catastrophic and irreversible. These side effects include sterility, early onset menopause, heart disease, increased stroke risk, cancer, early onset dementia, male pattern baldness, urinary tract dysfunction. See HERE:

And HERE4 for more details.
3. Oestrogen. Males are given high doses of oestrogen to bring on female characteristics. The male body softens into more of a female shape. However, the unwanted side effects include heart disease, increased stroke risk, cancer, early onset dementia. See HERE5 and HERE6 for more details.
The surgeries involve removing healthy breasts in an attempt to create a man’s chest, castrating males to try and create a vagina, breast implants for men, hysterectomies for females, construction of a fake penis out of skin and muscle from either the arm or the leg. Many of these surgeries are experimental and irreversible, with high risk of complications. See HERE7 for further details.
Schools that teach GII and/or support Social Transition may consider that they are removed from any harm that may eventuate to the child due to Gender Affirming Care.
But this may not be the case, given the nature of Gender Affirming Care. As mentioned above, the medical profession does NOT diagnose whether Gender Affirming Care is required. It is the child that makes that decision.
The question is How are schools helping the child to believe they are born in the wrong body so that they need Gender Affirming Care?
As discussed above, the evidence is mounting that Social Transition is a conveyor belt to Gender Affirming Care. Children spend most of their time at school. If GII and Social Transition are supported at school, it follows that the child will likely proceed to Gender Affirming Care. If GII and Social Transition are NOT supported at school, it also follows that the child will most likely grow out of any gender discomfort.
Each State and Territory in Australia have their own specific laws of negligence. However, there are enough similarities to provide a general analysis regarding whether schools are negligent in teaching GII to students and/or allowing Social Transition at school.
The question of whether the law of negligence applies to schools in this situation is determined by examining whether:
1. there is a duty of care;
2. there was a breach of the duty of care;
3. the breach of duty caused the damage or injury.
1. Duty of Care
Tort law, otherwise known as the law of negligence, creates a duty of care between certain people in society. It is a legal obligation to take care to avoid harming others. This legal duty of care does not arise in all circumstances. However, the Courts have held that the relationship of teacher/student has an automatic and undeniable duty of care.
The Courts have also held that this duty of care is non-delegable. Due to the concept of vicarious liability, this means that the school itself is liable for a breach of this duty by a teacher. Hence, schools have a duty of care to avoid their students being harmed. This has implications for the various Departments of Education in Australia.
2. Breach of Duty of Care
Whether a school has breached its duty of care to its students is determined by examining whether:
· the risk was foreseeable (that is, it is a risk of which the person knew or ought to have known);
There is now a significant body of evidence that demonstrates that Gender Affirming Care can cause catastrophic and irreversible damage to a child. This evidence includes:
a. testimonies from multiple people who have been harmed from Gender Affirming Care. This knowledge has been reported in the Australian media and is widely available to those who make even a cursory inquiry on the internet. For example, Channel 7 Spotlight Episode on Detransition,
the testimony of detransitioners in the US such as Chloe Cole, UK detransitioners such as Richie Herron,
b. the commencement of legal cases around the world, including Australia, against providers of Gender Affirming Care. For example, Isabelle Ayala, Richie Herron referred to above, Jay Langadinos, Luka Hein, Layton Ulery, Prisha Mosely.
c. the fact that many countries and states around the world are banning or restricting medical transition of minors due to such damage. Norway, Sweden, Finland, Denmark and the UK have restricted the use of puberty blockers and cross sex hormones for children. Over 20 US States have banned the medical transition of minors. This information is easily available on the internet. See below for an example.
d. an Australian health insurer (MDA National) has now stated it will not cover medical practitioners where a claim arises out of their assessment that a child is suitable for gender transition or them prescribing cross sex hormones for a child. See HERE8 for more details.
Accordingly, it is not unlikely that the Courts would find that the risk to a child of Gender Affirming Care, who has been instructed in GII and/or allowed to Socially Transition, is a risk that is easily identifiable if the teacher/school undertook basic internet research on the topic. It is unlikely that a school, in the normal course, would instruct students in a topic without examining that topic itself. Hence, there is a strong argument that such a school/teacher ought reasonably to have foreseen the risk of harm.
· the risk was not insignificant; and
The elements of whether the risk was “not insignificant” may be easily satisfied given the nature of Gender Affirming Care and the harm that arises from such “care.”
As discussed above, Gender Affirming Care prescribes that the medical practitioner merely “affirms” the patient’s decision that they have gender dysphoria and provides the necessary medications and surgeries that the patient would like to achieve medical transition. If a school has instructed a child in GII so that the child starts to think he/she is born in the wrong body, and that child proceeds to Gender Affirming Care, it is easy to see that the Courts may link the cause of that medicalisation and harm to the school. Likewise with Social Transition. Social Transition is a conveyor belt to Gender Affirming Care (see discussion above) and the Courts may easily link the harm caused to the child with Social Transition.
Thus, there is clearly a “not insignificant risk” that a child who decides that they are “trans” due to GII instruction and/or Social Transition at school, will most likely demand and receive the necessary medical intervention to enable transition.
· in the circumstances, a reasonable person in the person’s position would have taken precautions.
The question is whether a reasonable person would have taken precautions against the risk by ensuring that students were not instructed in the concepts of GII at the school and also that students were refused the ability to Socially Transition in the school environment.
In deciding this issue, the Court is required to consider certain things, including the probability that the harm would occur if care were not taken, the likely seriousness of the harm, the burden of taking precautions to avoid the risk of harm, and the social utility of the activity that creates the risk of harm.
Again, given the evidence showing that Social Transition is a direct pathway to Gender Affirming Care and the evidence demonstrating the catastrophic and irreversible damage that a child will suffer on that pathway, it is likely that these elements would be satisfied. Given schools have control over their policies of instruction and behaviour of students and that it is, in fact, a school’s job to instruct students in a safe manner, it would be hard to argue that a reasonable person would not take such precautions.
In relation to the burden of taking precautions, it would be difficult for a school to argue that NOT teaching something and NOT adding layers of bureaucracy to enforce Social Transition is a burden. With respect to the social utility of allowing GII instruction and Social Transition, the Courts may find that the banning of these activities happening around the World indicates that there is a strong movement against the transition of children.
3. Causation
A determination that negligence caused particular harm comprises the following elements:
· that the negligence was a necessary condition of the occurrence of the harm;
· it is appropriate for the scope of the person’s liability to extend to the harm so caused.
As discussed above, schools that instruct students in GII and/or allow students to Socially Transition during school are leading those students down a path that inevitably results in Gender Affirming Care. As there is now compelling evidence suggesting that Socially Transitioning a child is a conveyor belt to Gender Affirming Care, this leads to the conclusion that permitting Social Transition is a necessary condition of medical transition. Students spend a significant proportion of their time at school. There is a very strong argument that if Social Transition were prohibited by schools, the students would not be put on this pathway to harm.
Given that teachers and schools are required to provide a safe learning space for children, it would not be difficult to anticipate that a Court would find it appropriate for the scope of the liability of the school to extend to the harm. There is no undue burden on schools to NOT teach GII and to NOT allow Social Transition. In fact, it would reduce the burden on schools to remove these from the curriculum, policies and procedures.
Accordingly, the element of causation may not be difficult to satisfy.
That schools have been negligent in exposing children to gender ideology is currently being considered in the UK, the jurisdiction from which Australian negligence law derives. For example, parents are bringing a joint claim in negligence against the UK Department for Education for a failure to act on the foreseeable harms caused to children by gender ideology. (see Link HERE9). We suspect this will be the start of many negligence cases against schools and against Departments of Education in jurisdictions that have such a duty of care.
Note that the above is a general overview, and each case will be decided on its specific facts and unique characteristics. Contributory negligence will be a limiting factor and the statutory provisions most States and Territories have enacted will also play a role in the outcome. However, the risk to schools and the various Education Departments is high and should be carefully considered when a school decides to promote GII instruction and Social Transition.